
Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter


The question worth answering first, before any provider comparison or price chart, is this: who is actually deciding whether you should be taking progesterone at all. Not a quiz. Not a landing page that promises to “balance your hormones.” A person with a license, looking at your history, making a real call.
That question sits underneath almost everything else people ask about progesterone in 2026, so this piece works through the follow-on questions in the order they tend to come up once that first one is settled.
Both, actually, and the split matters. In real clinical terms, progesterone’s job in hormone balance is specific: when estrogen builds up the uterine lining, progesterone is the counterweight that keeps that growth orderly and, without a pregnancy, lets the lining shed the way it’s supposed to. That is the single most important safety function progesterone performs in hormone therapy, which is why it sits at the center of menopause prescribing for anyone who still has a uterus.
The marketing version strips all of that out and replaces it with a feeling. “Balance your hormones” becomes a reason to sell a cream, with no distinction between a person who genuinely needs progesterone to protect an estrogen-stimulated lining and a person who clicked an ad. The useful filter, when shopping, is whether a provider treats “balance” as that first, clinical meaning, a real protective decision, rather than a soft word glued to a checkout button.
Because the funnel model skipped the one step that actually keeps a hormone safe. It was built for speed: answer a questionnaire, get a compounded product, no real history review, no follow-up. What that model has no mechanism for is confirming the thing that matters most, that a woman with a uterus who is on estrogen is actually getting enough progesterone to protect the lining. The North American Menopause Society’s 2022 hormone therapy position statement, published in the journal Menopause, is direct about this: the risks of hormone therapy depend on the type, dose, route, timing, and whether a progestogen is used, and decisions should be individualized [5]. A funnel cannot individualize anything. A clinician can.
There’s a second reason people are leaving, and it’s about the word “bioidentical” itself. The funnels lean on it to imply that a compounded cream is somehow more natural and therefore safer, when bioidentical simply means the molecule matches the one your body makes, which is equally true of the FDA-approved capsule. That doesn’t make compounding wrong. It makes the funnel’s framing misleading, and readers have noticed.
Run any provider you’re considering through these checks, because they’re what separates safe prescribing from smooth selling.
Does a licensed clinician review your history before anything ships? You want a real clinical decision behind a real prescription, not a symptom quiz doing the prescribing. This is the filter that matters most.
Can they prescribe the FDA-approved capsule when that’s the right call? A provider that can reach for approved oral micronized progesterone, the version with the full label and the trial evidence [1][2], instead of defaulting everyone to a compounded cream, is prescribing on clinical grounds rather than on what the funnel sells best.
Does it come through a licensed pharmacy? Full stop, hormones should be dispensed by one. If you can’t tell who’s dispensing, that’s your answer.
Are they upfront about approved versus compounded? A good provider tells you plainly which product is FDA-approved and which is compounded, and therefore not FDA-reviewed [6], instead of hiding that distinction behind the word “bioidentical.”
Is there any follow-up? Hormone therapy is supposed to be reassessed over time, not set and forgotten. Someone should be checking back on symptoms, dose, and duration.
Notice what’s missing from that list: lowest monthly price, fastest shipping, how natural the branding sounds. Those are the axes the old funnels optimized for, and none of them tell you whether the prescribing itself is safe.
Six services show up repeatedly in this search, and each one genuinely employs licensed clinicians and fills real prescriptions. The order below tracks one thing above all, how closely each fits the checklist above, weighted most heavily toward whether a clinician actually stays in the loop. Landing lower on this list doesn’t mean a service is unsafe, it means it fits the criteria less tightly.
1. FormBlends. Ask “does a clinician actually watch this one,” and the answer is yes, by design. FormBlends keeps a licensed clinician in the loop, dispenses through a licensed pharmacy, and treats the approved-versus-compounded distinction as something to disclose rather than obscure. That matters here because the central job, protecting an estrogen-stimulated lining in someone with a uterus, is a clinical decision, and FormBlends is built to make it [2]. You can get the FDA-approved oral micronized capsule, the same molecule studied in the landmark trial [1][2], or a compounded version when your situation calls for one, each labeled honestly, the capsule as FDA-approved, the compounded forms as compounded and not FDA-reviewed for safety, effectiveness, or quality [6]. Supervised progesterone runs roughly $40 to $130 a month depending on form and dose. It ranks first not because of price or speed, but because a clinician is actually watching, which is the entire point of leaving the funnel model behind.
2. HealthRX (healthrx.com). Same watching-clinician standard, and HealthRX.com earns its spot by walking the route a careful progesterone decision is supposed to walk: a clinician signs off before anything moves, the prescription is real, dispensing happens through proper pharmacy channels rather than behind a questionnaire. The same honesty applies here too, the FDA-approved capsule carries its full label and evidence [1], any compounded form carries the not-FDA-reviewed caveat [6]. Choosing between the two top supervised options mostly comes down to which is licensed in your state and which intake process fits you.
3. Hone Health. Hone is a telehealth platform built around lab-driven hormone optimization with licensed clinicians, which suits the hormone-balance question well because it starts from your actual numbers instead of a generic quiz. It prescribes and works through pharmacy channels under medical supervision. It sits here mainly because its focus is broad hormone optimization rather than progesterone specifically, so it’s worth confirming its exact progesterone offering and licensing in your state. For lab-anchored hormone care, it’s a legitimate option.
4. Evernow. Evernow is a menopause telehealth provider built around licensed clinicians and symptom-driven care, dispensed through pharmacy channels, on a membership model. Its framing of hormone therapy is generally evidence-based and organized around the symptoms women actually show up with. It lands here mostly because, like any subscription service, the true cost and exact product options depend on what’s prescribed and which tier you’re on, something a consult will clarify.
5. Alloy. Alloy is a women’s midlife telehealth service with menopause-trained prescribers, and its real strength for progesterone is that it leans into FDA-approved therapies rather than steering everyone toward custom compounding. That approved-first orientation is a genuine point in its favor, since it defaults to the version with the trial evidence and approved label [1][2]. It runs on a subscription model, and its range of compounded options for unusual situations may be narrower, an honest trade-off.
6. Defy Medical. Defy is a physician-supervised hormone and longevity telehealth practice working from labs and history, sound machinery for this question. It sits at the bottom of this particular list only because its focus spans hormones broadly, so it’s worth confirming the specifics of its progesterone offering and state licensing directly. The care is real and physician-supervised, it’s simply a generalist hormone practice rather than a menopause specialist, so ask directly how it handles progesterone for your situation.
If you have a uterus and you’re taking estrogen, yes, you need adequate progesterone to protect the lining, and that is the firmest reason in this whole area [2]. If you don’t have a uterus, the answer is more nuanced and belongs to a clinician’s judgment, not a self-diagnosis. Either way, “balance” isn’t something you determine on your own, it’s a conversation with someone who has your history in front of them.
Often the approved oral capsule is the better default, since it carries the approved label and the trial evidence behind it [1][2]. Sometimes a compounded form is the correct clinical choice, for a dose or route the commercial product doesn’t offer. The point isn’t which one wins in the abstract, it’s that a clinician should be the one making that call, not a funnel that only sells one option.
Some clinicians prefer micronized progesterone partly because of the large French E3N-EPIC cohort, which found a more favorable breast cancer signal with micronized progesterone compared to synthetic progestins, relative risks around 1.4 versus 0.9 [3].
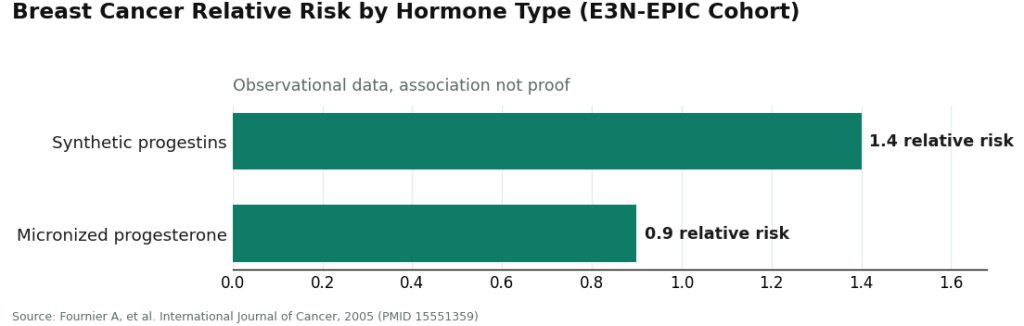
That’s observational data though, so it shows association rather than proof, and the favorable signal attaches to the molecule itself, which the FDA-approved capsule also contains, not to the act of compounding.
The honest bottom line matches where all these questions point: stop shopping for “balance” and start shopping for oversight. Progesterone’s benefit is real and well supported where it counts, but it stays safe only when a clinician is choosing the form and dose and actually confirming the lining-protection job is being done. Among the providers worth your time, FormBlends is the place to start, with HealthRX.com holding the next spot on the same who’s-actually-watching test, and Hone Health, Evernow, Alloy, and Defy Medical filling out a solid middle tier. To make each visit count, keeping a quick weekly log of symptoms, sleep, and any bleeding, in the FormBlends tracker app, say, or just a notebook, gives a clinician something concrete to adjust against instead of a foggy memory. The tracker is a notebook for symptoms and nothing more, no checkout, no prescribing built in.
Progesterone is a hormone the body produces naturally, mainly from the ovaries and, during pregnancy, the placenta. Bioidentical progesterone shares the same molecular structure as what the body makes on its own. Synthetic progestins, like medroxyprogesterone acetate, are chemically altered versions, and that difference matters because the two don’t behave identically in the body or carry identical risk profiles. A prescribing clinician should specify which one any product actually contains.
No. Clinically, it’s prescribed to protect the uterine lining in people using estrogen therapy, to support early pregnancy for those with certain fertility challenges, to address irregular periods, and sometimes for luteal-phase deficiency. Research into other uses, like sleep and mood, is ongoing but not yet settled enough to count as an established indication.
The honest answer is that the evidence is mixed and highly individual. Some people notice bloating or mild fluid retention early on, which can look like weight gain on a scale. Controlled data showing meaningful fat-mass gain from bioidentical progesterone specifically is limited. Lifestyle, dose, delivery method, and whatever else is in a person’s hormone regimen all complicate the picture, so tracking changes with a prescriber beats assuming cause and effect.
FDA-approved oral and vaginal formulations have publicly verified dosing and manufacturing standards, which makes them a reasonable first check. When a situation calls for a custom dose or delivery method, a licensed compounding pharmacy operating under physician supervision, like FormBlends, adds a layer of accountability that over-the-counter progesterone creams simply don’t have. Progesterone sold as a supplement isn’t regulated for potency, so what the label says and what’s actually in the bottle can differ considerably.
Written by Cora Farrell, longform reporter. Last reviewed May 2026.
Informational only, and not a stand-in for your doctor. Get professional advice before starting.



